

Could toenail zinc content assessed by portable X-ray fluorescence be a field friendly biomarker of zinc status? Professor David Fleming of Mount Allison University describes where the science is at.
Zinc deficiency is a widespread problem which has been associated with a variety of serious health effects. Diagnosing zinc deficiency at the individual level is, unfortunately, a somewhat thorny issue. Currently, there is no single method of determining zinc status which is both simple and reliable. The best option is probably the measurement of plasma (or alternatively serum) zinc concentration [1,2]. This approach, however, requires a sequence of non-trivial steps pertaining to the sample acquisition, storage, and analysis (usually at a distant lab). Other reliable or potentially useful biomarkers of zinc status have been noted, including zinc concentration in urine and hair [1,2]. These approaches also have drawbacks.
Zinc concentration in nail was recently described as an “emerging biomarker” by the Biomarkers of Nutrition for Development (BOND) zinc expert panel [2]. This designation indicates that nail zinc concentration has a theoretical association with zinc status, but requires further study. This need for additional development was reinforced in a Technical Brief from IZiNCG, which provided an overview of assessing zinc exposure using hair or nail zinc [3].

Toenail clippings ready for measurement by portable X-ray fluorescence (Photo: David Fleming)
We recently conducted a study involving the measurement of zinc concentration in toenail clippings using two different methods: portable X-ray fluorescence (XRF) and inductively coupled plasma-mass spectrometry (ICP-MS) [4]. Of the two methods, portable XRF is a relatively new approach to zinc biomarker analysis, while ICP-MS may be considered a “gold standard”. We measured single toenail clippings from 60 different individuals living in Atlantic Canada (the population was drawn from the Atlantic PATH cohort [5]). The clippings were measured first by portable XRF, a non-destructive technique, and then by ICP-MS. The population average zinc concentration was found to be 85 µg/g from ICP-MS. The portable XRF technique was very sensitive to detecting zinc in the clippings and provided a reasonable estimate of zinc concentration. Using the XRF output spectrum to determine a normalized zinc signal, we found a correlation coefficient r = 0.68 between the XRF results and the ICP-MS zinc concentrations. Looking forward, correlation between the two methods might be improved by measuring multiple points on each clipping when using XRF – in our study, only a single point on each clipping was assessed by XRF.

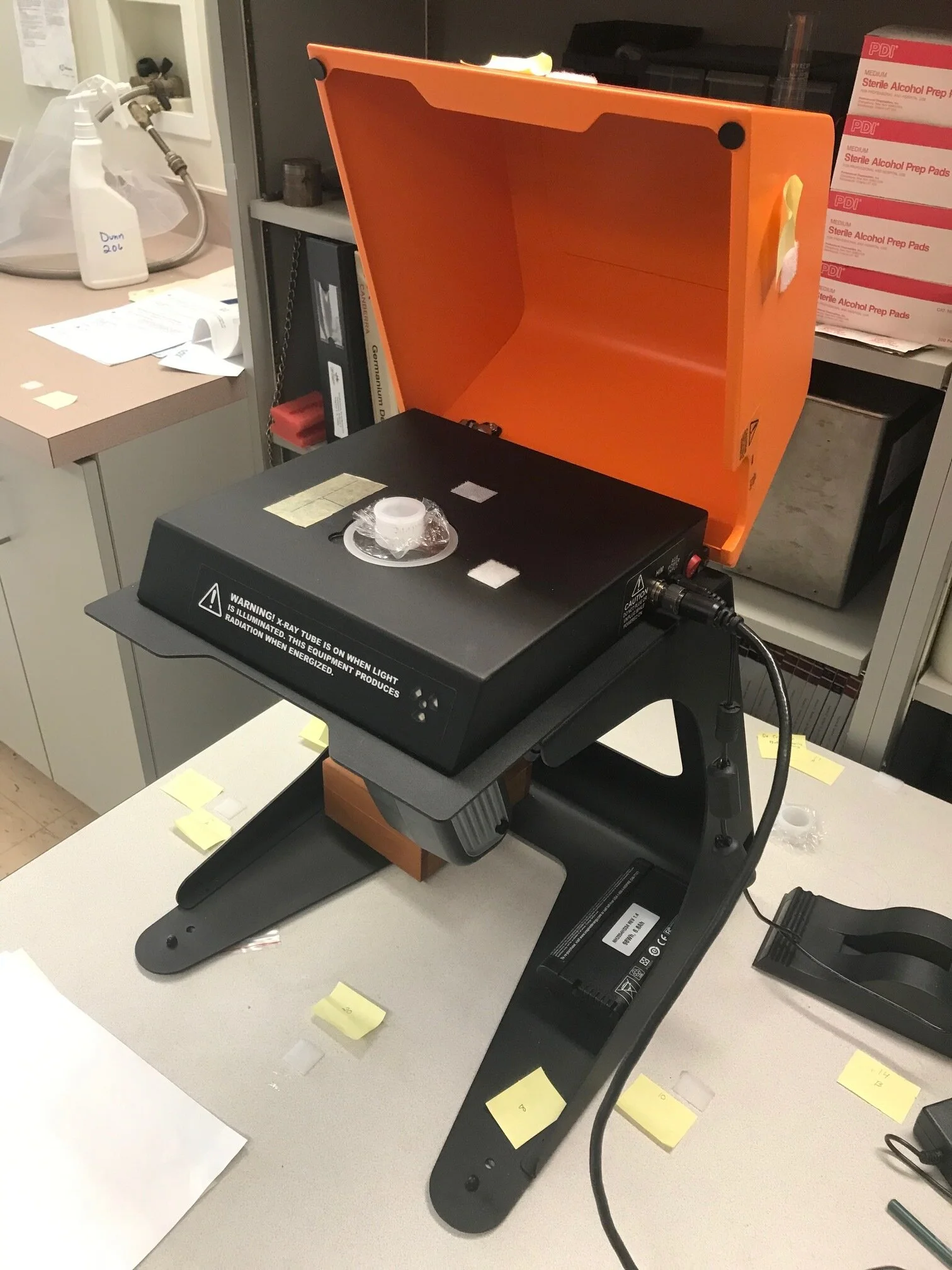
Single toenail clipping in portable X-ray fluorescence instrument (Photo: David Fleming)

Single toenail clipping (Photo: David Fleming)
The portable XRF approach presents a number of potential advantages for the analysis of zinc concentration in nail clippings. Measurements could be made in a field setting and results provided quickly. Sample preparation is minimal, operating conditions are simple, and the technique is relatively inexpensive. If the correlation of XRF results with ICP-MS concentrations could be improved, portable XRF might therefore be an especially attractive approach for assessing zinc concentration in nail clippings. The other critical issue here, of course, is whether zinc concentration in nail is truly representative of an individual’s zinc status. That remains an open question which will require additional study to resolve. If zinc concentration in nail is eventually upgraded from “emerging biomarker” to “useful biomarker”, we anticipate that portable XRF will receive a great deal of attention and become a potentially important component of public health initiatives targeting zinc deficiency.
References
[1] N.M. Lowe, K. Fekete, T. Decsi, Methods of assessment of zinc status in humans: a systematic review, Am. J. Clin. Nutr. 89 (2009) 2040S-2051S.
[2] J.C. King, K.H. Brown, R.S. Gibson, N.F. Krebs, N.M. Lowe, J.H. Siekmann, D.J. Raiten, Biomarkers of nutrition for development (BOND) – zinc review, J. Nutr. 146 (2016) 858S-885S.
[3] International Zinc Nutrition Consultative Group (IZiNCG) Technical Brief No. 8, Assessing population zinc exposure with hair or nail zinc (2018), https://www.izincg.org/technical-briefs
[4] D.E.B. Fleming, S.L. Crook, C.T. Evans, M.N. Nader, M. Atia, J.M.T. Hicks, E. Sweeney, C.R. McFarlane, J.S. Kim, E. Keltie, A. Adisesh, Portable X-ray fluorescence of zinc applied to human toenail clippings, J. Trace Elem. Med. Biol. 62 (2020) 126603.
[5] E. Sweeney, Y. Cui, V. DeClercq, P. Devichand, C. Forbes, S. Grandy, J.M.T. Hicks, M. Keats, L. Parker, D. Thompson, M. Volodarsky, Z.M. Yu, T.J.B. Dummer, Cohort profile: the Atlantic partnership for tomorrow’s health (Atlantic PATH) study, Int. J. Epidemiol. 46 (2017) 1762-1763i.








































